Features of Exposure Doses to the Public due to the Fukushima Accident
Abstract
Many attempts to evaluate exposure doses to the public have been made since the Fukushima accident. Doses to the public from external exposures have been found to be more significant than those from internal exposures. Initiating restrictions on consumption of contaminated foods and drinks fairly promptly after the accident is thought to have helped. Fukushima Prefecture estimated the maximum external effective dose for the first four months after the accident at 25 mSv. Additional external effective doses of Fukushima residents in recent years have all been evaluated at within several mSv per year. Residents are not expected to receive large additional external doses after returning to the evacuated areas after the evacuation orders are lifted. NIRS has estimated the maximum thyroid dose due to inhalation of I-131 in the early phase of the accident at around 30 mSv, which corresponds to an effective dose of 1.2 mSv. Committed effective doses due to internal exposure from radiocesium intake have been estimated to be notably smaller than 1 mSv as a whole. Estimated exposure doses during the early stages of the accident have certain inevitable uncertainties for both internal and external exposures, and further investigation to reduce these uncertainties is urgent.
Key words: effective dose, exposure dose, external exposure, internal exposure, thyroid dose
1. Introduction
One significant concern after the Fukushima Nuclear Power Plant (NPP) accident has been exposure doses from radionuclides deposited on ground and from the radioactive plumes in the early stages of the accident. Many studies have been conducted since the accident on the effects of the accident in terms of exposure doses to the public, evaluating exposure doses by different methods. These studies have explored the features of exposure doses originating from the accident. Evaluation of exposure doses, however, must continue till the environmental effects of the accident become negligible. Further, exposures in the early stages of the accident from radionuclides with short half-lives such as iodine (I)-131 have not been thoroughly clarified. Studies and evaluations of these aspects of exposure doses must be performed for a long time. In this report, some of the main dose evaluation activities carried out so far will be introduced to give an overview of exposure doses to the public. While not intended to cover all related activities, the selected results can sketch a good view of the present status of evaluated exposure doses to the public.
In this report, exposure doses are basically expressed in terms of the effective dose, which is a whole-body exposure dose taking radiation sensitivity of important organs and tissues into account (ICRP, 2007). Only in Section 4.1 will exposure doses be discussed regarding thyroid doses according to the cited documents. The duration of exposure dose evaluations vary from case to case: four months, one year, and the committed effective dose is defined as an effective dose integrated over 50 years for adults and up to the age of 70 for children after their intake of radionuclides. Further, throughout this report, the additional exposure dose, defined as the exposure dose due to radionuclides released from the Fukushima accident, will be considered. In other words, the dose contribution from natural radiation will be excluded from the evaluated dose in any case.
2. Exposure Pathways in the Environment
Radionuclides released into the atmosphere during an accident are first transported by air and are a source of external exposures to the public from the sky. People who breathe these radionuclides suffer internal exposures designated as “inhalation.” In the early stages of the Fukushima accident, diverse radionuclides existed in the atmosphere including noble gases, such as xenon (Xe)-133 and krypton (kr)-85, which are not deposited on ground, and also short-lived radionuclides which are difficult to detect later (IAEA, 2015). Nuclear reactor analyses estimate a lot of radionuclides to have been released during the Fukushima accident. For technical reasons, however, there were few cases of these short-lived radionuclides being directly measured in the environment. Thus, knowledge on radionuclides soon after the accident and the related exposure doses still has some uncertainties which need further investigation.
Some radionuclides released into the atmosphere are deposited on the ground or other environmental materials through dry and/or wet deposition according to precipitation amounts. The deposited radionuclides become a source of external exposures. According to past experience with large nuclear accidents such as the Chernobyl accident, the radionuclides deposited on various environmental media are anticipated to exist in the environment and continue to be a source of exposures to the public for a long time. Taking into account the length of exposure time, exposures from deposited radionuclides are generally more important than exposures from radioactive plumes, which disappear in a short time.
If the deposited radionuclides wind up in foods, and inhabitants eat the contaminated foods, it results in internal exposures defined as “ingestion.” Contamination of foods can occur by various pathways. For example, edible plants such as leafy vegetables may be contaminated by direct deposition and also by uptake of radionuclides through their roots; drinking water is contaminated by direct deposition into water reservoirs and by dissolution of radionuclides deposited upstream of them. Animals and fish can ingest radioniclides through the complex food chains existing in biotas.
In case of the Fukushima accident, restriction of contaminated foods started fairly early and has been continued on the basis of reliable and extensive screening for a wide range of foodstuffs. Therefore, it is thought that internal exposure doses to the public have been smaller than external exposure doses. In this context, the situation differs considerably from that of the Chernobyl accident, where the effective doses to the public due to internal exposures were comparable to those due to external exposures (UNSCEAR, 2008).
3. External Dose Evaluations
Three trials are introduced here which evaluate external exposure doses covering a wide time range from the accident till the near future when relocated inhabitants will return. In most cases where dose evaluations have been carried out, no significant external exposure doses due to the accident have been reported.
3.1 Evaluation for the First Four Months
Since air dose rates in the early stages of the accident were much higher than in later periods, external exposure doses to the public have been a significant concern together with inhalation. Fukushima Prefecture has evaluated external exposure doses during the first four months after the accident in the Fukushima Health Management Survey, aiming for comprehensive health examinations for all inhabitants of Fukushima Prefecture (Ishikawa et al., 2015). Dose evaluations were carried out using a dose evaluation system developed by the National Institute for Radiological Sciences (NIRS) (Akahane et al., 2013) based on the results of questionnaire surveys of the inhabitants.
Questionnaires were delivered to the inhabitants of Fukushima Prefecture to investigate the detailed behaviors of each inhabitant during the four months. Responses to the questionnaire were used to reconstruct personal trails for the four months on a map. At the same time, daily air dose rate maps were created using monitoring data if any reliable ones existed; otherwise, evaluated dose data based on atmospheric transport simulation were utilized. By superimposing the personal trail and the time-dependent air-dose-rate maps, the accumulated external exposure dose for each inhabitant could be evaluated.
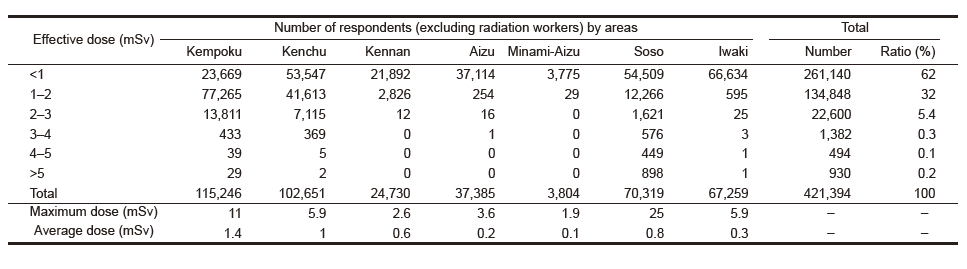
Evaluated external exposure doses for 421,394 residents are tabulated in Table 1. The evaluated dose data were classified by district in Fukushima Prefecture. The maximum dose and the average dose for all the residents were estimated at 25 mSv and 0.8 mSv, respectively. The doses for 99.4 percent of all responders were estimated at less than 3 mSv.
Table 1 Maximum and average external exposure doses for the first four months estimated from the Fukushima Health Management Survey (Ishikawa et al., 2015).
3.2 Measurements Using Personal Dosimeters
After the Fukushima accident, many local municipalities started measuring individual doses using personal dosimeters. Soon after the accident, the measurements focused on children and pregnant women thought to be sensitive to radiation. With passing time, the targets of the measurements were expanded to whole generations. Each municipality has carried out a large number of measurements from several thousand to several tens of thousands each year.
Personal dosimeters were originally designed to evaluate exposure doses of workers in facilities but not exposure doses of inhabitants in living environments. Therefore, personal dosimeters are designed for conservative evaluation of effective doses in working environments, and the response of personal dosimeters in environments contaminated by radiocesium has not been well investigated. The NIRS and the Japan Atomic Energy Agency (JAEA) examined the response of personal dosimeters in contaminated fields in the Fukushima region, and also at a calibration facility using standard gamma-ray sources (NIRS & JAEA, 2014, 2015). Different commonly used models of personal dosimeters all turned out to give readings close to the effective dose for all ages.
Figure 1 shows the distribution of external exposure doses evaluated on the basis of personal dosimeter measurements in Fukushima City in 2014. Most of the evaluated doses in Fukushima City in 2014 were less than 1 mSv. Temporal changes in the frequency distribution of external exposure doses in Sukagawa are shown in Fig. 2. The doses have obviously decreased with time. Similar tendencies have been observed for other municipalities.
JAEA has conducted measurements with personal dosimeters independently from the measurements by municipalities, and the results have been analyzed taking behavior patterns of the subjects into account (Takahara et al., 2015). According to an analysis of about 500 cases in Fukushima City till August 2015, it turned out that 1) the external exposure dose distribution is subject to a log-normal distribution; 2) inhabitants that spend relatively longer times outside tend to receive higher doses; 3) the distribution of doses evaluated based on behavior patterns and local air dose rate data can reasonably reconstruct the observed distribution.
-
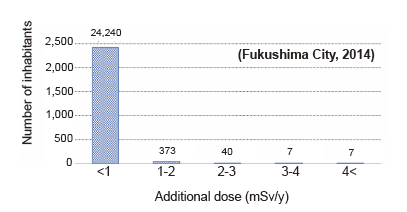
Fig. 1 Estimated distribution of annual external exposure doses in Fukushima City in 2014 based on measurements using personal dosimeters. (Fukushima City, 2015).
-
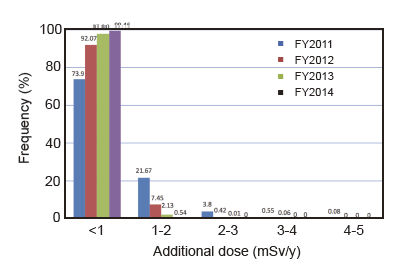
Fig. 2 Estimates of temporal changes in frequency of annual external exposure doses in Sukagawa based on measurements using personal dosimeters. (Sukagawa City, 2015)
3.3 Evaluation of Returning Inhabitants
The evacuation orders are being lifted one after another, and the relocated inhabitants are gradually returning to their homes. Expected exposure doses after their return are essential information in deciding on their return. Measurements using personal dosimeters cannot be applied to inhabitants who will return to home in the future. Meanwhile, exposure doses estimated using currently used simple evaluation methods based on air dose rates tend to include large uncertainties. To solve these problems, JAEA devised a method of evaluating external exposure doses using interviews and detailed air dose rate measurements.
First, the returning inhabitant is interviewed about his or her life patterns expected after the return. In this interview, a concrete personal trail that the inhabitant will follow each day is examined, including length of time spent in each place. Then, air dose rate measurements are carried out along the expected personal trail using a KURAMA-Ⅱ system able to obtain air dose rates and GPS positional data every three seconds (Tsuda et al., 2015). The measured air dose rates are integrated over one day along the personal trail, weighted by the time length, then converted to effective doses by multiplying with dose conversion factors (Saito & Petoussi-Henss, 2014; Satoh et al., 2016), considering the age of the targeted inhabitant. Thus, the total external exposure dose per day is obtained along with details. Postulating several different patterns for each person, the doses are summed over a year resulting in the annual external exposure dose. The dose contribution from natural background gamma rays can be directly estimated using spectral information from KURAMA-Ⅱ (Andoh et al., 2016).
Hitachi Solutions East Japan Ltd. (HSE) technically supported by JAEA have conducted dose evaluations using this method. The results obtained for the municipalities of Katsurao, Kawamata and Tomioka in FY2015 are shown in Fig. 3 (NRA & HSE, 2016). In about 70 percent of all cases, the evaluated annual external exposure doses were less than 1 mSv, and in all cases the annual doses were smaller than 3 mSv. It was found that the external exposure dose can differ by several times according to the individual, even if living in the same area. This suggests that local distributions of air dose rates and life patterns drastically affect external exposure doses.
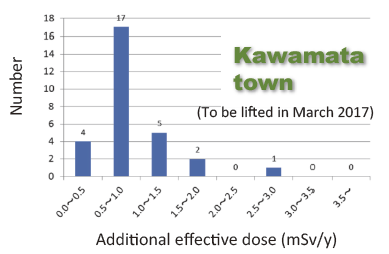
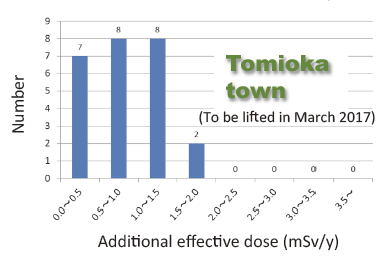
Fig. 3 Estimated external exposure doses for residents returning to areas where evacuation orders will be lifted.(NRA & HSE, 2016).
4. Internal Dose Evaluations
Three important cases of internal exposure dose evaluations in terms of thyroid doses and effective doses are presented. The first case concerns thyroid dose reconstruction for I-131 by integrating different information; the others are committed effective dose evaluations for radiocesium based on results of whole body measurements and on radiocesium concentrations in foodstuffs. It was confirmed that as a whole, the internal exposure doses in terms of effective doses were smaller than external doses.
4.1 Thyroid Doses from I-131
Though inhalation exposures from I-131 in the early phases of the accident are considered important, there is a lack of basic information on I-131 concentrations and intake from the environment because of its short half-life, leading to large uncertainties in dose evaluations. Kim et al. (2016) evaluated thyroid doses, integrating various available information for all of Fukushima Prefecture. There exist about 1,000 cases where I-131 activity in the thyroid was directly measured in children by one means or another. In such cases, the measured data were used directly in dose evaluation. Additionally, in cases where direct iodine measurement data did not exist, whole body measurement data on radiocesium intake were utilized for about 3,000 adults. Iodine-131 intake for these inhabitants was estimated by assuming the concentration ratio of I-131 to Cs-137 differed with region. Further, in cases where no measurement data were available, results of atmospheric transport simulation were used for dose estimation.
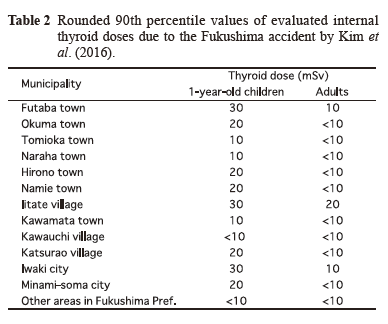
Table 2 provides rounded 90th percentile values of evaluated internal thyroid doses in different municipalities. The estimated highest thyroid dose was 30 mSv for one-year-old infants in the municipalities of Futaba, Iitate and Iwaki. It must be noted that a thyroid dose of 30 mSv corresponds to a 1.2 mSv effective dose. These results are consistent with preceding studies (Tokonami et al., 2012; Matsuda et al., 2013). Large uncertainties, however, may be included in estimated thyroid doses since information directly related to I-131 is limited. Some follow-up projects are underway, given the situation and importance of I-131 doses.
Table 2 Rounded 90th percentile values of evaluated internal thyroid doses due to the Fukushima accident by Kim et al. (2016).
4.2 Committed Effective Doses Based on WholeBody Measurements
A large number of inhabitants have undergone whole body measurements since the accident to determine their body burdens of radiocesium. Whole-body measurement of radiocesium is a well-established method, and radiocesium body burdens have been estimated with small uncertainties. Momose et al. (2012) evaluated committed effective doses (CED) for about 10,000 inhabitants based on whole body measurements carried out by January 2012. The inhabitants were mostly from eleven towns in Fukushima Prefecture. The observed maximum body burden of radiocesium (Cs-134 and Cs- 137) was 2.7 kBq for children less than eight years old and 14 kBq for adults. The actual intake scenarios, that is, when and how the radiocesium was taken into the body, were not known, but acute intake via inhalation was assumed, leading to a conservative evaluation.
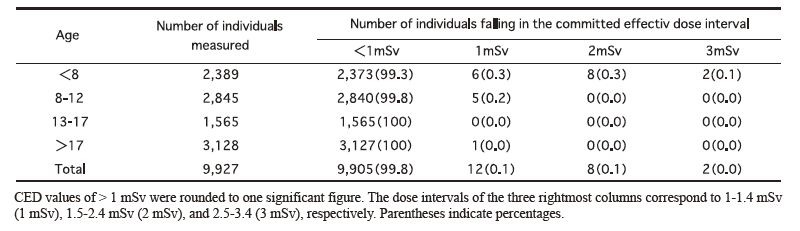
Table 3 provides a summary of estimated CEDs. The CEDs for 99.8 percent of inhabitants were estimated to be smaller than 1 mSv. The 50 percentile value of CED was 0.025 mSv for inhabitants over 17 years in age, and the maximum CED was less than 3 mSv. Whole body measurements have been carried out continuously even after the report, and no significant intake of radiocesium has been reported.
Table 3 Committed effective dose distribution of residents from eleven towns in Fukushima Prefecture, measured by JAEA from July 11, 2011 to January 31, 2012. (Momose et al., 2012).
4.3 Committed Effective Doses Due to Dietary Intake
Radiocesium concentrations in various foodstuffs have been extensively screened to check if they exceed the restriction limits. The screenings have shown the number of foodstuffs exceeding the limits to decrease with time. Committed effective doses from foods circulating in the market have been evaluated using a market basket method in which various foodstuffs are purchased and cooked according to dietary statistics in the targeted area (Uekusa et al., 2014; Tsutsumi et al., 2013). Also CEDs have been evaluated by a duplicate diet method where samples identical to the diets actually consumed by inhabitants are measured (Uekusa et al., 2014; Hirokawa et al., 2016). According to these studies, CEDs from dietary intake have been confirmed to be much smaller than 1 mSv. This proves that extensively performed screening has been working effectively.
5. Summary
The large-amount of radionuclides released from the Fukushima accident have resulted in exposures to the public. External exposures are thought to have been more significant than internal doses from the Fukushima accident, since restriction of foodstuffs started soon after the accident and has been conducted effectively. Various activities have been carried out since the accident to evaluate exposure doses to the public. In this article, some important examples of dose evaluation after the accident have been introduced, and it was not intended as a review of all important activities concerning dose evaluation. This article’s contents are considered sufficient to grasp an outline of dose evaluations carried out and the range of evaluated exposure doses both for external and internal exposures. In conclusion, no significant exposures leading to obvious radiation effects have been observed so far. The evaluated maximum effective dose is around several tens of mSv for external exposures and around several mSv for internal exposures. For both external and internal exposures, the maximum dose was thought to be due to exposures in the early phases of the accident. Because detailed information on exposures in the early phases is still lacking, certain uncertainties in the evaluated doses undoubtedly exist. Thus further efforts to clarify exposure doses in the early phases are needed. Also, it will be essential to keep up efforts to protect inhabitants from excess exposure from deposited radionuclides, and keep monitoring the health of the inhabitants till the effects of the accident become truly negligible.
References
- Akahane, K., S. Yonai, S. Fukuda, N. Miyahara, H. Yasuda, K. Iwaoka, M. Matsumoto, A. Fukumura and M. Akashi (2013) NIRS external dose estimation system for Fukushima residents after the Fukushima Dai-ichi NPP accident. Scientific Reports, 3: 1670. doi:10.1038/srep01670.
- Andoh, M., N. Matsuda and K. Saito (2016) Evaluation of air dose rates owing to natural radioactive nuclides in Eastern Japan by car-borne surveys using the KURAMA-Ⅱ. Transactions of the Atomic Energy Society of Japan. (accepted)(in Japanese)
- Fukushima City (2015) Summary of Glass Badge MeasurementResults in Fukushima City in FY2014. (in Japanese)
- Hirokawa, D., S. Omori, N. Nishimura, K. Yoshida, I. Wada and A. Yamakoshi (2016) Survey of radioactive cesium and potassium intake from food using duplicate diet (Fiscal Year 2011–2014). Food Hygiene and Safety Science, 57: 7–13.
- IAEA (International Atomic Energy Agency) (2015) The Fukushima Daiichi Accident, Technical, Vol. 1: Description and Context of the Accident. ISBN:978-92-0-107015-9.
- ICRP (International Commission on Radiological Protection) (2007) The 2007 Recommendation of the International Commission on Radiation Protection. ICRP Publication, 103.
- Ishikawa, T., S. Yasumura, K. Ozasa, G. Kobayashi, H. Yasuda, M. Miyazaki, K. Akahane, S. Yonai, A. Ohtsuru, A. Sakai, R. Sakata, K. Kamiya and M. Abe (2015) The Fukushima health management survey: estimation of external doses to residents in Fukushima Prefecture. Scientific Reports, 5: 12712. doi: 10. 1038/srep12712.
- Kim, E., O. Kurihara, N. Kunishima, T. Momose, T. Ishikawa and M. Akashi (2016) Internal thyroid doses to Fukushima residents— estimation and issues remaining. Journal of Radiation Research, 57(Suppl 1): i118-i126.
- Matsuda, N., A. Kumagai, A. Ohtsuru, N. Morita, M. Miura, M. Yoshida, T. Kudo, N. Takamura and S. Yamashita (2013) Assessment of internal exposure doses in Fukushima by a whole body counter within one month after the nuclear power plant accident. Journal of Radiation Research, 179: 662–668.
- Momose, T., C. Takada, T. Nakagawa K. Kanai, O. Kurihara, N. Tsujimura, Y. Ohi, T. Murayama, T. Susuki, Y. Uezu and S. Furuta (2012) Whole-body counting of Fukushima residents after the TEPCO Fukushima Daiichi Nuclear Power Station accident. Proceeding of the 1st NIRS Symposium on Reconstruction of Early Internal Dose, NIRS-M-252, 67–82.
- NIRS and JAEA (National Institute of Radiological Sciences, Japan Atomic Energy Agency) (2014) Research on the Characteristics of Personal Doses after the TEPCO Fukushima Dai-ichi Nuclear Power Plant Accident. NIRS-M-270. (in Japanese)
- NIRS and JAEA (2015) Additional Research to “Research on the Characteristics of Personal Doses after the TEPCO Fukushima Dai-ichi Nuclear Power Plant Accident.” NIRS-M-276. (in Japanese)
- 1NRA and HSE (Nuclear Regulation Authority, Hitachi Solutions East Japan, Ltd.) (2016) Continuous Measurements of Air Dose Rates Postulating Patterns of Living Activities. (in Japanese)
- Saito, K. and N. Petoussi-Henss (2014) Ambient dose equivalent coefficients for radionuclides exponentially distributed in the ground. Journal of Nuclenr Science and Technology, 51: 1274– 1287.
- Satoh, D., T. Furuta, F. Takahashi, A. Endo, C. Lee and W.E. Wolch (2016) Age-dependent dose conversion coefficients for external exposure to radioactive cesium in soil. Journal of Nuclenr Science and Technology, 53: 69–81.
- Sukagawa City (2015) Results of Individual Dose Measurements in FY2014. (in Japanese)
- Takahara, S., M. Iijima, K. Shimada, T. Kushida and Y. Shiratori (2015) Development of deterministic approach to assess doses to the public from external exposures in the areas contaminated by the Fukushima Daiichi Nuclear Power Station accident. JAEA-Research, 2014-024.
- Tokonami, S., M. Hosoda, S. Akiba, A. Sorimachi, I. Kashiwakura and M. Balnov (2012) Thyroid doses for evacuees from the Fukushima nuclear accident. Scientific Reports. 2:507. doi: 10. 1038/srep00507.
- Tsuda, S., T. Yoshida, M. Tsutsumi and K. Saito (2015) Characteristics and verification of a car-borne survey system for dose rates in air: KURAMA-Ⅱ. Journal of Environmental Radioactivity, 139: 260–265.
- Tsutsumi, T., H. Nabeshi, A. Ikarashi, A. Hachisuka and R. Matsuda (2013) Estimation of the committed effective dose of radioactive cesium and potassium by the market basket method. Food Hygiene and Safety Science, 54: 7–13.
- Uekusa, Y., H. Nabeshi, T. Tsutsumi, A. Hachisuka, R. Matsuda and R. Teshima (2014) Estimation of dietary intake of radioactive materials by total diet methods. Food Hygiene and Safety Science, 57: 177–182.
- UNSCEAR (United Nations Scientific Committee on the Effects of Atomic Radiation) (2008) Sources and effects of ionization radiation. UNSCEAR 2008, Report to the General Assembly with Scientific Annexes, Volume Ⅱ, Scientific Annexes D.